A 75-year-old patient came to the emergency department complaining of left hemithorax pain and worsening dyspnea. The pain had relation to the breathing cycle. Neither fever nor chills were present as well as a recent fall or respiratory infection. Patient´s history includes Parkinson´s disease.
The patient was conscious, well-oriented to time and space and afebrile. Breathing was superficial, tachypnoeic, with no breath sounds and only minimal hemithorax excursions on the left side. Breathing on the right side was clear over the whole lung. Blood oxygen level dropped below 90 % without oxygen support. Atrial fibrillation with HR of 91 bpm, blood pressure 118/76 mmHg.
Shortly after examination, the heart rate increased to 140-160 bpm, administration of fluid and amiodarone followed.
At admission, lab tests revealed increased levels of inflammatory markers and renal insufficiency: CRP 270, leucocytes 24 000, 93 % of neutrophils, creatinine 270 umol/l, urea 18 mmol/l.
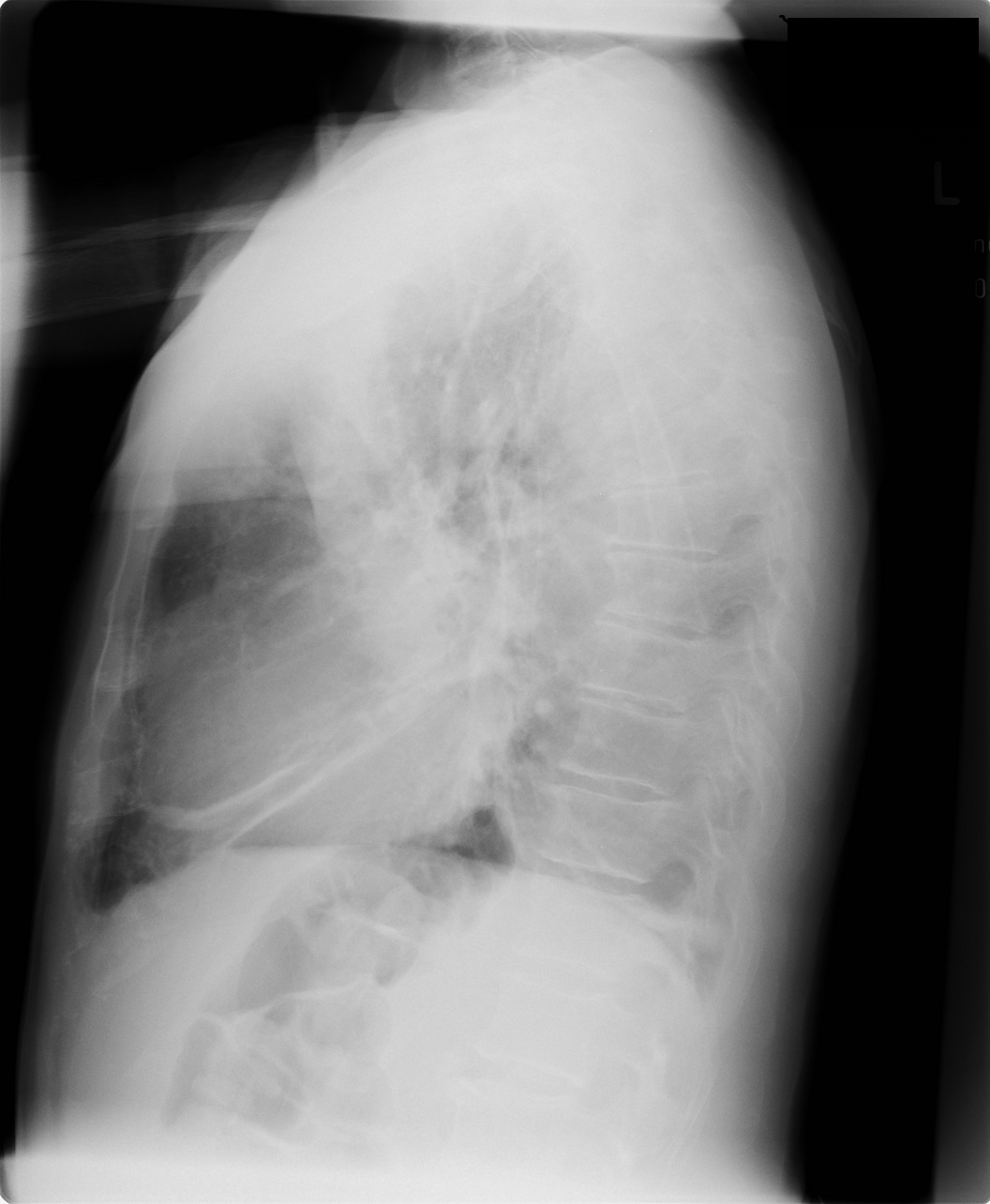
Chest X-ray at the admission:

Diagnosis: severe community-acquired pneumonia on the left side. Differential diagnosis encompasses thoracic empyema, sepsis.
Blood cultures were taken, and empiric antibiotic therapy was started.
Chest CT was performed, and the patient was admitted to ICU.
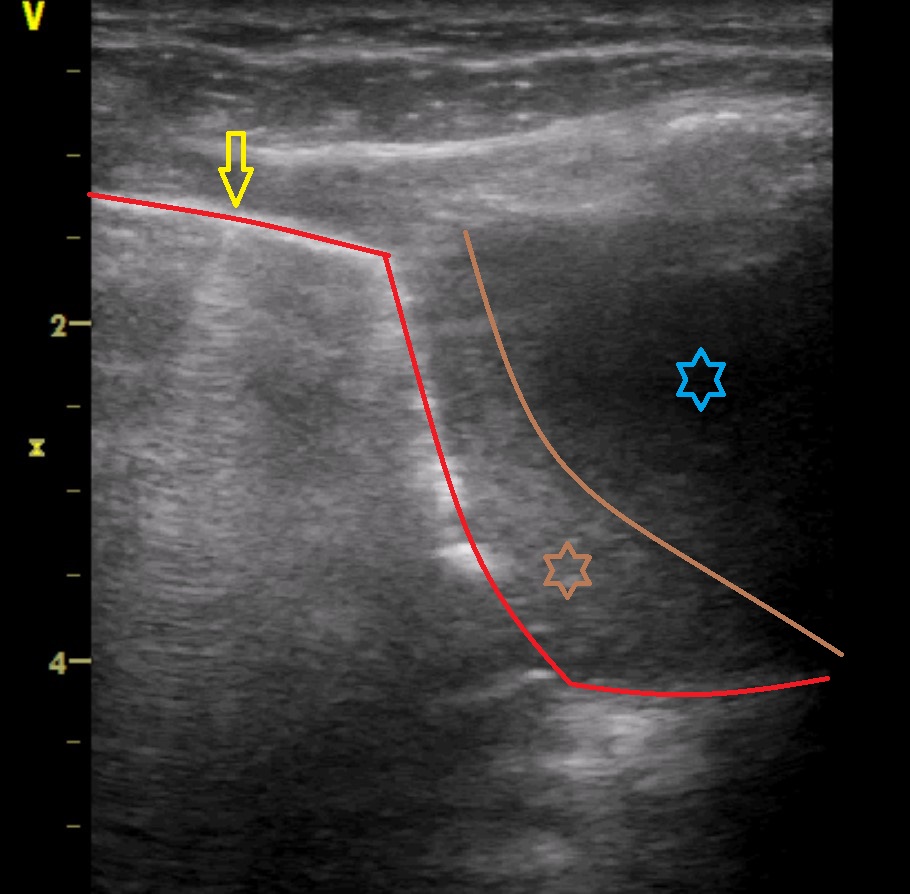
Ultrasonography of the left hemithorax was performed: