
A male patient was admitted to the hospital fever exceeding 39 °C lasting one day and a new onset of haemodynamically significant atrial fibrillation with a rapid ventricular response. His history includes diabetes and nephrectomy on the left side for a tumour. CRP 96 mg/l, procalcitonin negative, leucocytes 17 600.
He complained of chest pain and strangury. Admission ultrasonography (heart and chest) at emergency did not reveal any pathology. Neither clinical nor X-ray signs of respiratory infection were present. Heart rate decreased after administration of a bolus of amiodarone and crystalloid solution. Symptoms withdrew.
Admission to the ICU followed.
There is no medical report of previous abdominal ultrasonography; I was just told that there were no signs of obstruction of the urinary tract. Check ultrasonography of the right kidney was performed 2 hours later after above-mentioned ultrasonography performed in the emergency department:

Oblique scanning plane at the right posterior axillary line below the caudal rib
The right kidney is visualised at its longitudinal axis; its upper pole becomes visible during inspiration. Dilation of renal pelvis and calyces (yellow colour) – grade II hydronephrosis. Red colour marks renal contour and boundary between renal sinus and parenchyma. Brown colour marks rib with acoustic shadow below it.
Oblique scanning plane at the right posterior axillary line below the caudal rib
The right kidney is visualised at its longitudinal axis; its upper pole becomes visible during inspiration. Dilation of renal pelvis and calyces, especially in the region of inferior pole – grade II hydronephrosis.
The probe was rotated by 90° in anticlockwise direction:
Oblique scanning plane at the right posterior axillary line below caudal rib, the mark is placed cranially
The right kidney is visualised at its transverse axis; its upper pole becomes visible during inspiration. Dilation of calyces in the region of both poles, renal pelvis is superimposed by acoustic shadow below colon (full of air) – grade II hydronephrosis.
History of the patient was completed during ultrasonography – the patient complained of episodic back pain in the region of the right kidney.
Conclusion: solitary kidney, grade II hydronephrosis, suspicion of acute bacterial pyelonephritis concerning clinical symptoms.
Early negative ultrasonography does not exclude obstruction of the urinary tract. Check ultrasonography should always be performed after administration of fluid to a patient in severe condition. The obstructive cause can be revealed after the restoration of diuresis.
Recommendation: taking urine and haemoculture for microbiological examination, empirical antibiotic therapy, consultation with a urologist concerning maintaining the maximum urine derivation in a patient with a solitary kidney. Check ultrasonography was recommended in this case as well as CT (to clarify the position of obstruction) in the case of persistence of congestion.
On the next day, the patient did not complain of any difficulties and was afebrile. Diuresis was abundant with microscopic hematuria. Inflammatory markers raised (CRP 306 mg/l, procalcitonin 0.82 ng/ml, leucocytes 18 500). Spontaneous restoration of sinus rhythm.
Check ultrasonography of the right kidney was performed:

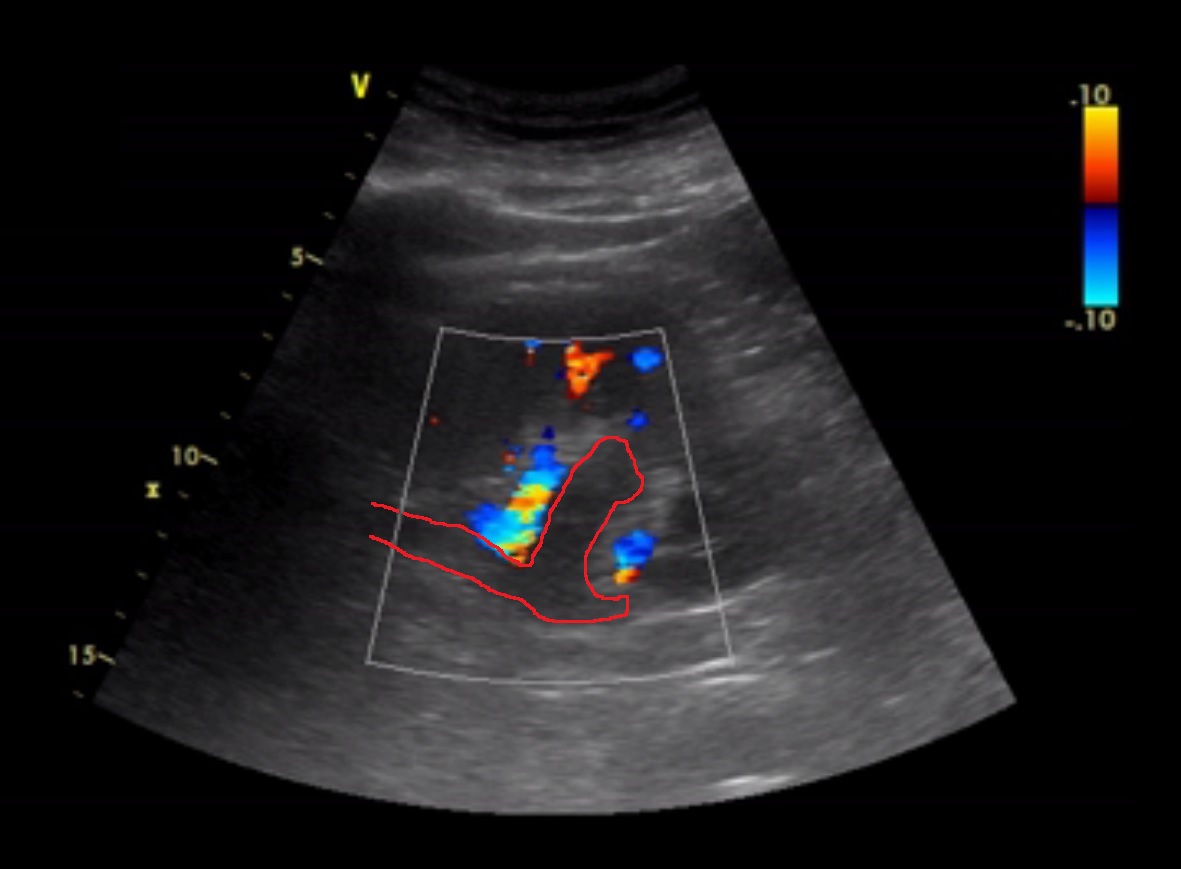
Oblique scanning plane at the right posterior axillary line below caudal rib, CFM
The right kidney is visualised at its longitudinal axis; its upper pole is superimposed by acoustic shadow. Dilation of renal pelvis and calyces, especially in the region of inferior pole – grade II hydronephrosis.
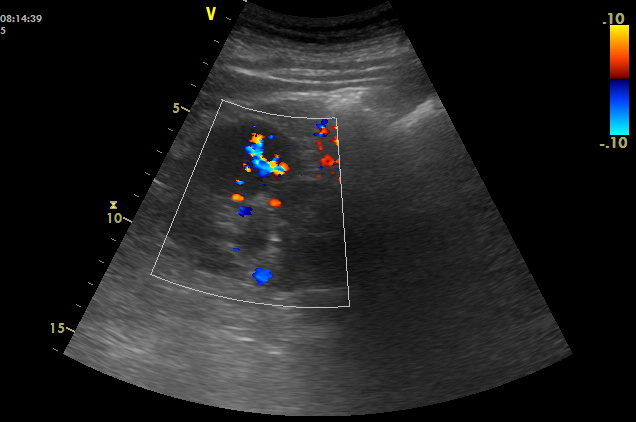

Oblique scanning plane at the right posterior axillary line below caudal rib, CFM
The right kidney is visualised at its transverse axis. Dilation of the renal pelvis with propagation to the calyces (these show a minimal dilation in this recording).
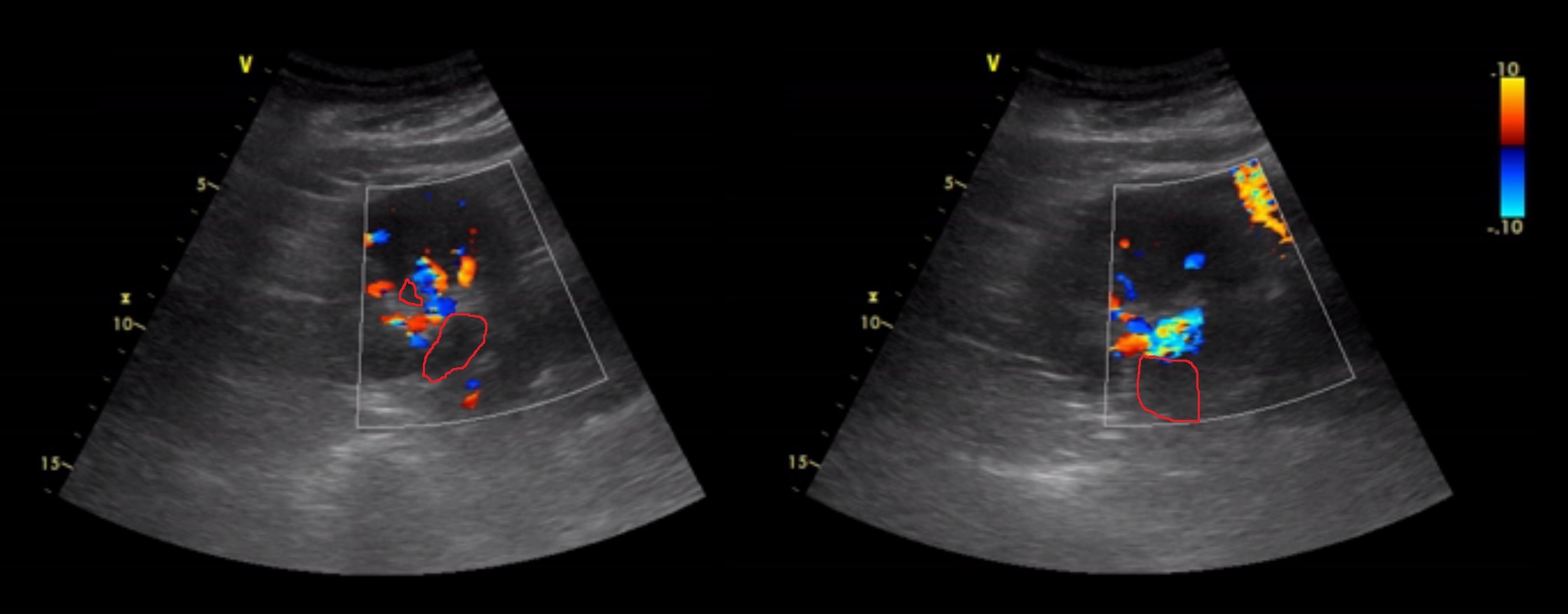
Oblique scanning plane at the right posterior axillary line below caudal rib, CFM
The right kidney is visualised at its transverse axis. Dilation of the renal pelvis with propagation to the calyces (these show minimal dilation in this recording).
Conclusion: dilation did not show any progress, grade I-II hydronephrosis.
CT revealed small ureterolithiasis at the place where ureter crosses the iliac vascular bundle. Short dilation of ureter above this stone was also found. The patient was transferred to the urological department for placement of a D-J stent.