Let´s suppose you admit a patient to your ICU for circulatory collapse and dyspnea. During auscultation, you hear coarse wet phenomena suggesting a significant amount of mucus in airways. Chest X-ray performed during admission revealed bilateral infiltrations and high inflammatory markers were found in lab tests. You conclude the patient as having septic bronchopneumonia.
However, something does not fit. Patient´s history includes ulcer of ascending aorta with partial dissection (conservative therapy) and repetitive sepsis (MSSA). Concave upward ST elevations in all leads were found in admission ECG. Why?
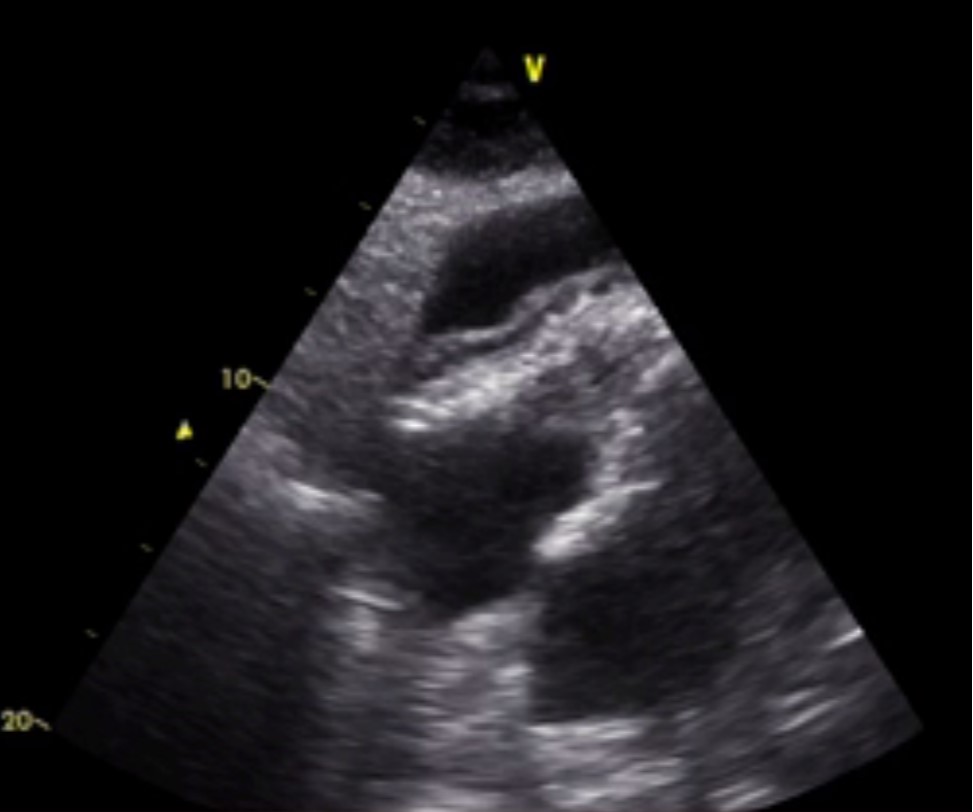
You perform echocardiography.
The patient is examinable only at S4C projection with the following findings: